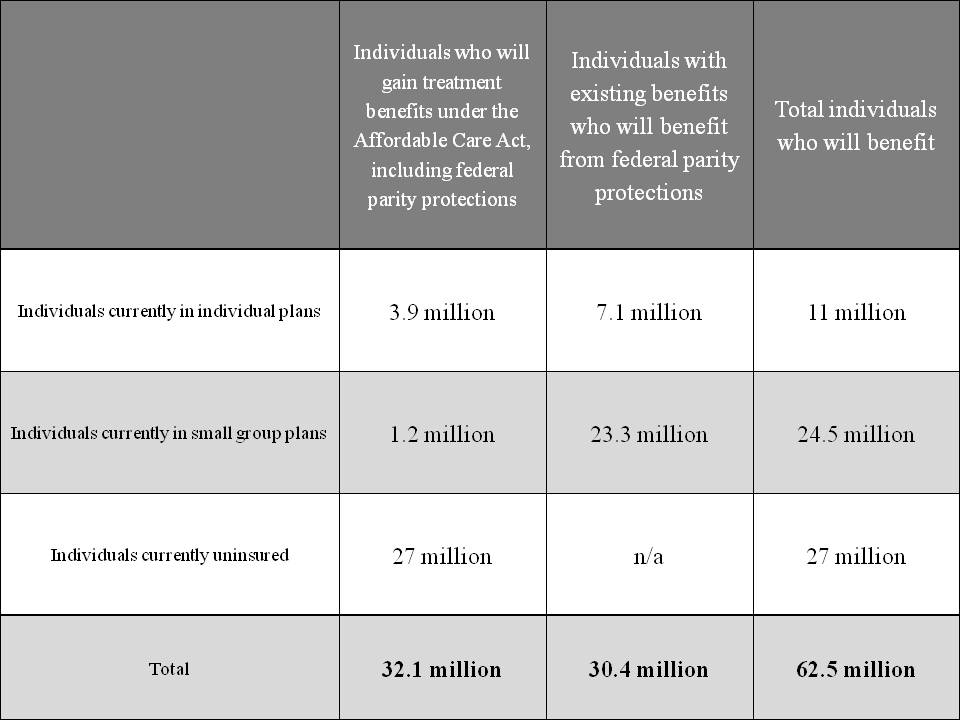
Given how often some people demand “health-oriented drug policy” from the Obama Administration it is more than a little peculiar how one of the biggest reforms in history didn’t attract more attention and draw more praise in the blogosphere. With the Administration’s declaration that treatment of mental health and substance use disorders are essential health care benefits, to be provided not only in the state health insurance exchanges but in all new individual and small-market health insurance plans, over 60 million Americans just got better insurance coverage for these disorders. The graphic below is from HHS:
That isn’t the end of the good news. The more than 100 million Americans who receive coverage under large-group plans are also getting better coverage due to the Mental Health Parity and Addiction Equity Act. Passed in the waning days of the G.W. Bush Administration with the regulations being written by the Obama Administration, the law mandates that any offered benefits for addiction and mental health must be comparable to those offered for other conditions.
But wait there’s more: Medicare, which enrolls almost 50 million people, has long had inferior coverage for addiction and mental health outpatient care, reimbursing only 50% of costs versus 80% of those for other forms of medical care. Thanks to a provision in the 2008 Medicare Improvements for Patients and Providers Act (again, give it up for the 110th Congress and President Bush), this disparity in reimbursement is being phased out and will be entirely eliminated by January 1 of next year.
When you consider that addictions almost always evidence themselves in adolescence or early adulthood, it becomes clear that the ACA provision allowing parents to keep children on their insurance until age 26 adds yet another layer of protection for the population.
Some people of course have coverage from more than one of the above sources, but even granting that overlap, over 200 million Americans have gotten improved insurance coverage for treatment of drug and alcohol problems (and mental health disorders as well). This includes many people who were starting with nothing, as well as a large population that had a benefit of inferior quality.
This is the biggest expansion to access to care for addiction in at least 40 years and probably in American history. In financial terms, it is certainly the biggest commitment of public and private resources to the health care of people with substance use disorders in U.S. History. Congratulations are in order to countless grassroots advocates, civil servants, political appointees, members of Congress and two U.S. President for transforming the face of health care for addiction.
No explanation for the “marijuana” tag?
Let me offer one. If the Obama administration finally accepted the fact that marijuana does have important, safe, and effective uses in medicine, it would reschedule marijuana at the federal level and cease pointless federal enforcement efforts against it. That would benefit all 300+ million Americans.
Sorry, doesn’t work that way. Even if it were legally possible to make a drug schedule III without approving it as a medicine, it remains the case that a schedule III drug is illegal unless prescribed, and it can’t be prescribed unless the FDA has approved it. So there’s no short-circuit around the process of actually doing the clinical trials. (I agree that the Administration is culpable for not getting the regulatory machinery out of the way of the research process.)
Whatever marijuana’s uses as medicine, most of the people buying it in California are buying it to get stoned, not to treat their ailments. Allowing medical use still leaves a large recreational market.
There are good arguments for legalizing non-medical uses, but it would be nice if advocates stopped dragging the “medical” red herring across the trail.
Plenty of things are illegal, but almost never prosecuted. (Which is why we’re not having this conversation from prison cells.) There’s no reason in principle why pot couldn’t join this category, though it would obviously be better (From an avoidance of enabling abusive selective prosecution.) to just “unschedule” it, and get the federal government out of the business of telling people what they can smoke.
Perhaps I was too constrained in my verbiage. While I do support federal rescheduling of cannabis to facilitate access for patients, I actually believe outright legalization would be preferable to medicalization. Legalization wouldn’t mean cannabis is any less effective in treating a range of medical conditions.
Lower down, paul commented on the extra medical costs of treating addiction, etc. In my case, I have synringomyelia. Cannabis is the only thing that’s really been effective in treating the intraspinal pain and other symptoms. I took care of that on my own until an “incident” took that away — at no cost to the state or the private insurance companies that the ACA helps subsidize (I am an advocate of national health care as the best alternative.) After some back and forth, I’m now on dronabinol/marinol (artificial THC) at a cost to the state of about $2500/month, which is maybe half as effective as natural cannabis and treats only the pain, not other symptoms, and a spectrum of other drugs with cost and side effects wholly out of proportion to their benefits.
I would be much better off with access to what I know works best. Presuming I was allowed to resume taking care of cultivating my own medicine, there would be about a >95% drop in my drug costs. I realize this is just one anecdotal case, but the math is striking and the benefits of better treatment are clear. We’d all be better off with less government meddling and greater support for alternatives in our healthcare system.
A straight question. Has anyone looked at the possibility that the exceptionally US high health care costs may be due in part to untreated addictions and mental health problems? It’s easy to think of scenarios where this is likely: self-harming behaviours like sharing needles or reckless driving, failure to seek medical help for treatable conditions at an early stage, not keeping appointments or complying with treatment regimens. Good care for addictions and mental health doesn’t make these issues go away, but it must reduce their impact.
No particular reason to think that addiction is any more common, or any worse treated, here than elsewhere. Remember that most addiction is to alcohol, and the U.S. is not an especially heavy-drinking country.
Oh? With at least 32 million Americans who up to now have not had health insurance coverage for addiction treatment?
I take your point that it would need a lot of untreated US alcoholism to balance the higher booze consumption (+ universal health care) of say Scotland.
Harold’s post and my comment also relates to mental illness.
There seems to be a rather conspicuously missing column, “Individuals who had benefits who will lose them as a result of the ACA”. One should, after all, always look at costs when looking at benefits, and this is far from a non-zero category, given the perverse incentive to reduce employee hours below 30 to avoid having to pay more expensive benefits, and the number of cases where the increased cost of insurance has driven people to go without.
Also, I heard it made some people turn gay. And anti-gun
“..and the number of cases where the increased cost of insurance has driven people to go without.”
I thought there was an individual mandate (with the subsidies) to prevent exactly this?
Draw up your column. Find some credible numbers, not hypotheses. I’ll not hold my breath.
Yeah, there’s a fine if you go without.
“In 2014, the penalty will be no more than $285 per family, or 1% of income, whichever is greater. In 2015, the cap rises to $975, or 2% of income. And by 2016, it reaches $2,085 per family, or 2.5% of income, whichever is greater.”
You might note that, for many people, maybe most, this maximum fine will be, even in 2016, substantially less than the employee contribution if they opt for health insurance. (I had to pick the ‘cheap’ insurance this year, and it was still more than that fine.) Which means if you’re choosing between the health insurance and feeding your family, you’re going to opt for paying the fine.
Granted, the fine probably means that you end up without health insurance AND living on instant ramen. It DOES manage to make a painful decision hurt even more. But I don’t think the ACA, “Obamacare” was ever intended to work. It was just meant to destroy the health care insurance market, so that people would have no choice but to accept the creation of a single payer system.
Are there good numbers for the uptake of mental health and addiction services by various classes of covered people? Traditionally there’s been a barrier because of potential adverse job and housing effects from using such covered services, but I don’t know how that might apply to new populations.