The universe of people obsessed with my Twitter debates with Michael Cannon presumably went ecstatic over our weekend exchange, which centered on Cannon’s short Friday column: “Your Friday afternoon news dump: Obama admin. Admits Medicaid expansion costs more than projected.â€Â Michael and I disagree on everything. He is the Cato Institute firebrand who has apparently dedicated his life to destroying the Affordable Care Act. But he is a smart guy. I often learn from what he writes even as I disagree with it.  Cannon quotes from a recently-released Medicaid actuary report, which bears careful reading.
Michael’s first sentence made my heart sink: “It appears that Medicaid-expansion enrollees are going to cost the states a lot more than they thought.†Given the current knife fight over getting states to expand their Medicaid programs, this would be quite damaging. We know, for for example, that behavioral health costs are significant in a subset of new enrollees. There are also complicated interactions with other state and federal assistance programs. It’s certainly plausible that Medicaid expansion will turn out to be more costly than originally thought.
Because he is such a firebrand happy warrior, I have learned to follow up on his hotlinks to see what else might be going on. So I hunted down the report and ran the numbers. The actuaries did indeed predict higher costs—but almost all in the first year when states wouldn’t have to pay any of these costs. (The higher costs seem to reflect pent-up demand and perhaps more pregnant women than predicted in this particular Medicaid pool. I would like to learn more about what’s happening as states gain experience in the expansion population.)
I also ran the actual numbers from this year and last-year’s reports. The increase in predicted annual* costs per enrollee are shown below, broken down between the states and the federal government. The increased cost to the states averages that Michael warns us about are…. about $5/enrollee per year between 2014 and 2022. If you’re having trouble finding it, its the blue line visually indistinguishable from zero. To Michael’s credit, he’s told me he will modify the post. He certainly should.
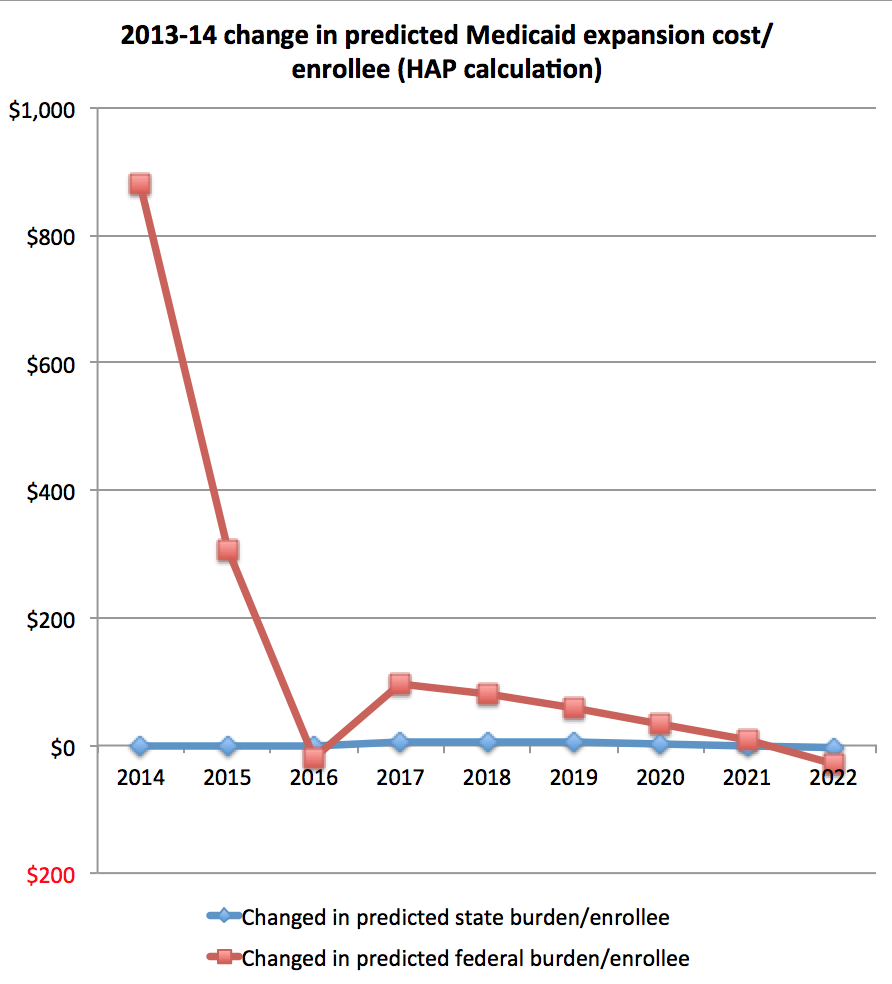
The increased costs to the federal government are shown in red. The difference here is about $881 in the first year as the Medicaid expansion gets rolling, and then plunges in subsequent years, averaging out at about $95/enrollee per year. Â That’s something like 2.2% of average non-disabled adult Medicaid costs. Despite the initial upward bump, things are quite manageable. It’s certainly not the sort of bad news one must conceal in a Friday news dump.
The main good news  about the overall Medicaid program is below the fold. Continue reading “Another false alarm on the costs of Medicaid expansion”