Victoria, British Columbia is trying to figure out how to deal with an encampment of homeless people who have serious substance use problems. Most homelessness is caused by rents being too high and wages being too low, but in this case the encampment is next to a shelter with empty beds, warmth, food and bathrooms (but presumably no allowance of substance use). The people quoted in the story seem baffled by why the homeless people are not using the shelter, but as the essence of addiction is prioritization of substance use over matters of basic biological necessity, they really shouldn’t be surprised at all (especially not Dr. Perry Kendall, who is a smarter guy in person than he comes off in this story — bad quoting by the reporter maybe).
The bottle gang under the bridge or on skid row, the heroin shooters who camp out by the train tracks, the methamphetamine and crack addicts clustered in burned out housing are each a portrait of human misery and a call to action for the rest of us. Quite frequently cities respond by starting a predictable cycle. Tolerance is the order of the day at first, live and let live. As adverse health and social consequences increase, service professionals are sent in to ameliorate the damage. Finally, the problem gets even worse and the police are sent in to shut the whole thing down, cracking heads as necessary.
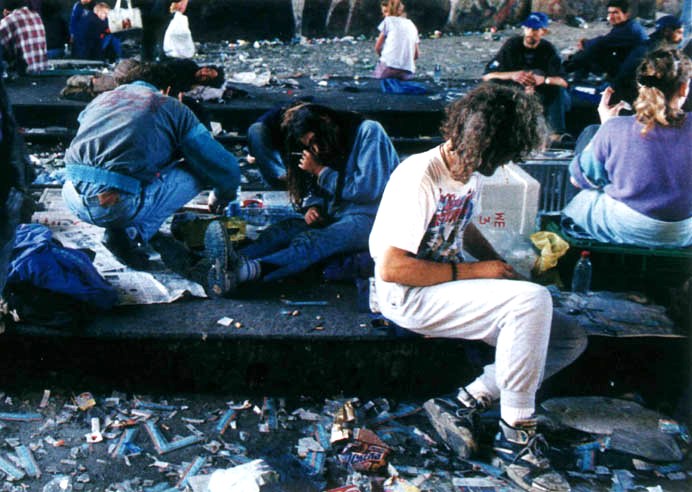
The needle park in Platzspitz in Zurich, Switzerland is the emblematic case. The park was declared a drug tolerance zone for the hundred or so addicts who were initially there. More addicts gathered over time, and public urination and defecation, prostitution, and petty theft became common. The city responded by providing services in abundance: needle exchange, methadone dispensing, safe sex education and a variety of other social services. But the problem didn’t get better. It got worse. At its peak, several thousand drug users/sellers a day were either in the park or passing through, and Platzspitz became completely unsafe both for the users and for everyone else. This photo captures the scene
Finally, the fed up local residents agitated for a crackdown and the police closed up the park. The addicts were dispersed and continued to both experience and to cause suffering around Zurich for many years.
There is no questioning the goodwill or humanity of a doctor who stitches up the face of a homeless alcoholic who has had a bottle smashed over her head, or a social worker who gives out a condom and safe sex advice to someone who is prostituting him or herself for drugs. Neither is there a basis to question the decency of a police officer who acts to stem public health and safety risk when encampments of addicted homeless people swell to an enormous size. The trap cities seem to fall into though is using only one of these responses and one set of agencies at a time. The problem is handed off in frustration to a new set of professionals who know how to do one specific thing, so they do it. It’s almost like a mother who after trying unconditional love all day with a difficult child says to the father as he returns home: “I’m sick of this and I want nothing more to do with this little brat. Slap some sense into him!”.
I wonder if any RBCers are aware of a case where public safety and public health professionals tried to handle one of these encampments together. I personally would like to see arrests made in the cases of prostitution/drug dealing/assault/petty theft with the arrestees put into mandatory abstinence programs akin to 24/7 Sobriety or Project HOPE, with services offered contemporaneously for medical, psychiatric, housing, employment and dental problems. Just a carrot will not do it, and neither will just a stick. And neither will a pile of carrots suddenly withdrawn and replaced with a pile of sticks.




{kind=link}
One question is why the shelters insist that clients come in sober. I understand not tolerating bringing drugs in, or outlandish behavior, but the case for “low-threshold” shelter - where someone can come in zonked at midnight and still get to sleep warm - seems strong.
Mark
There is a definitely a humanitarian case for getting grossly intoxicated people into warm shelter, particularly in Northern cities where alcoholic homeless people are at great risk of hypothermia every single winter, and deaths from exposure are shamefully common. There are at least two risks that shelters face though (and remember, most shelters are shoestring operations) when they let intoxicated people in to sleep it off: (1) Someone intoxicated and initially calm becomes violent unexpectedly and hurts another resident or staff and (2) Someone who comes in intoxicated wakes up in acute withdrawal and there is a medical emergency which many shelters are not equipped to handle.
As a Victoria local, I feel obliged to point out a factual error in the opening paragraph. The encampment is across the street from a facility that provides lots of important services for the homeless, but that is only open during the day. There are other availabe shelter beds elsewhere in the city, but they are not close at hand.
Hi Blake
Not sure what the factual error is, the news story explicitly mentions beds are available…don’t forget when much of this population sleeps. But in any event, and granting that it would be better if the facility had night hours at well, do you see anything on the ground that encourages you that your city will respond effectively?
Read the news story more carefully - the beds at Our Place are not currently funded - the facility is closed all night. The available beds are elsewhere in the city.
I’m not forgetting when they sleep - at night. This is not a theory, this is first hand knowledge of that specific location.
I am sorely disappointed with the behaviour of Mayor Fortin, and agree with the general premise of your article. It is just that specific detail that isn’t correct.
(Not mentioned in the Globe & Mail article: Two days ago the city council announced deliberations on a new by-law to push this camping into less obvious places, after the courts having declared they couldn’t just outlaw it completely.)
I just realized the other probable point of confusion. The Globe article doesn’t explain that the camping is already outlawed from 7am-7pm, and the police have been aggressively enforcing that ban. This means the only time the tents are setup there is exactly when Our Place is closed.
Blake
I yield to your personal knowledge obviously and appreciate you adding detail not in the article. Do you think though that night hours at the shelter would solve the problem, or just kick it down the road?
Keith
That depends what you mean when you say, “the problem”, doesn’t it? Would funding Our Place to be open 24/7 solve the entire substance abuse/mental health/homelessness problem in Victoria? Certainly not. Would it solve the ‘problem’ of the group of people camping out on the boulevard on that stretch of Pandora Ave? Absolutely.
Our Place is closer the sort of solution you are proposing than you might realize from the Globe article. They are not primarily a “shelter”. They have a good working relationship with the local police. In fact, they were one of the big proponents of the plan for the Vancouver Island Health Authority to buy the adjacent building from St. John’s Ambulance and run a new fixed needled exchange program there along with a 24/7 staffed police unit in the same building. Sadly, the “not in my backyard” brigade seems to have squashed those plans.
The fact that Platzspitz was a mess doesn’t prove that noncoercive provision for addicts is always inferior to coercion. (Neither is a final or sufficient solution.) Likewise the fact that homeless people may camp out even in sight of shelter. (I take Blake’s word about Victoria, but it’s a commonplace that some homeless people prefer to avoid shelters, which they may find frightening, depressing, or humiliating. You might, too.)
Coercive treatment can’t just be a matter of just marrying existing public-health or social-services initiatives w/ the police. Homeless addicts will be unlikely to present themselves to shelters, works vans, etc, that are seen to collaborate w/ people who’re out to arrest them. (One reason addicts defer emergency room visits, even to the point of disaster, is that they fear arrest — which does occasionally happen.) If you want voluntary points of contact with this population to survive, some will have to be kept at arm’s length from coercion. This may require some duplication of capacity.
In talking about “the problem,” be clear about the distinction between the addict’s medical interests, which may justify coercion, & the interests of others or of society, which are the usual people call the police. If you tell an addict you’re subjecting her to pain for her own good, but in fact are seen mostly to be trying to keep her off other people’s lawns, or if you’re unclear about the distinction, she’ll sense bullshit & you’ll have missed your shot.
Blake, I should resign and make you the blogger, great information and ideas on this. Thanks Keith
Part of the problem with many of the situations you describe is that the drugs themselves are still black market (alcohol’s a different story, of course). I believe that expansion of the swiss experience with clinic-style heroin maintenance programs are much more effective than simply providing a safe place to shoot up the uncertain street drugs (which is itself still better than nothing).
Certainly, there are some drug addicts who may require some kind of stick and those can be easily identified by the non-drug crimes they commit. Unfortunately, the stick is usually applied to all addicts, when a large number merely need an opportunity to re-focus their life without the constant street search from criminals for the drug they need. These are more likely to respond to a low-stress solution (something that the criminal justice system cannot provide).
Get a life, Pete. Your positions are untenable, unscientific, and inhumane. The CJS can be made to work well, and your alternative of legalization will do litter to ameliorate the destruction of drugs, and even drug markets, since underground markets will not simply go away under legalization.
As a member of Law Enforcement Against Prohibition, I would like to echo Guither’s comments. We need to explore regulatory alternatives to drug prohibition. It is interesting that the author of this post raised the issue of the Needle Park in Switzerland, but he did not discuss the public policy that evolved from that failed experiment. Platzspitz was shut down in 1992. In response in 1994 the authorities launched a prescription heroin trial program. It was successfully expanded and fourteen years later, in 2008, 68% of Swiss voters formally approved the prescription heroin program in a nation wide referendum.
Keith closes his post by saying, “I wonder if any RBCers are aware of a case where public safety and public health professionals tried to handle one of these encampments together.” However, in Victoria there is already an integrated community court. Police officers are already seconded to mental health teams and assertive community treatment (ACT) teams. (This is all publicly available information. Just google Victoria Integrated Community Outreach Team, Victoria Integrated Court, Victoria Integrated Mobile Crisis Response Team, etc.)
The issue is not cooperation. The issue is the open air drug markets created by prohibition.
David
During Prohibition, many homeless encampments and skid row areas centered on alcohol addiction.
After Prohibition, many homeless encampments and skid row areas center on alcohol addiction.
Keith
The reason I excepted alcohol in my post is that you can’t treat different drugs as if they have the same dynamics. For heroin, the clinic maintenance model is outstanding. It wouldn’t work for alcohol. It’s like calling marijuana and heroin illicit drugs as if they were the same thing.
And Keith, regarding your point about the fact that many homeless encampments and skid row areas centered on alcohol addiction both during prohibition and after prohibition, I’m not sure what value that has, since alcohol possession and consumption were legal during both periods. I also don’t quite frankly know whether, in those situations, alcohol came first, or homelessness and despair came first. I suspect a mix, with an emphasis on the latter.
Part of the trick is that we have to stop lumping all drugs together and trying to treat them with the blunt sledgehammer of prohibition. In a proper legal framework, each drug would have a different regulatory system that is designed to minimize harm. In the case of marijuana, that may be simply an age/place/situation regulation. In the case of heroin, it may be a tightly controlled clinic arrangement, but one that still shuts off most of the profit to the black market. Alcohol is a unique drug and poses its own set of problems which we can try to minimize, but not eliminate. I highly recommend Transform’s “Blueprint for Regulation” as a look into a world after prohibition. http://www.tdpf.org.uk/blueprint%20download.htm
I am glad to hear that you recognize that all drugs can’t be treated the same. So, which drugs are you against legalizing?
Let’s reverse it. One of the problems with these discussions is that some people assume that the default position is illegal, when that is not the case at all.
I am against criminalizing any drug. In other words, I am against using the criminal justice system to deal with the use of any drug at all. Criminalize things such as theft or assault, but not drugs. I am, however, in favor of different kinds of regulations and controls for different kinds of drugs. Even drugs that can cause death, like aspirin, should be legal, but with warnings and safety controls. Some drugs should be controlled so that you have to go to a doctor to get them. But no drug should be criminalized.
Truly, you have a dizzying intellect